
What if your financial donation could pave the way for improving donor and recipient matching, advancing novel cell-based therapy to increase the long-term success of organ transplantation, drug minimization, and even lead to recognition in a Nobel Prize summary?
That’s the power of the Organ Donation and Transplant Research Foundation of British Columbia (ODTRF).
The ODTRF provides grant funding through several programs, including the annual Venture Grant which funds new areas of study, as well as the Team Grant and Research Challenge which provide funding for patient-identified priorities.
And on a day that celebrates giving, we want to thank you.
The ODTRF is excited to share that we have recently achieved a milestone: $1 million in grants awarded to B.C. investigators! All because of you: those who have given, who have seen the value in transplantation and organ donor research in British Columbia, who understand the necessity of seed funding to advance organ donation and transplant science.
To celebrate, we want to share some highlights of what has been achieved, thanks to your generosity and belief in something better in the world of transplant and organ donation.
Tailoring Tregs: A New Way to Make Protective Immune Cells
When Dr. Megan Levings, a scientist at BC Children’s Hospital Research Institute, learned about CAR T-cell therapy – an advanced form of cancer treatment that involves genetically engineering a patient’s own immune cells to specifically target and destroy cancer cells – an idea started to percolate.

“I was keen to explore if the same could be done with T regulatory (Treg) cells,” explains Megan. “Was it possible to apply this same principle from cancer therapy to transplant, and develop Tregs that could specifically stop harmful immune response to transplanted organs?”
In 2011, Megan applied to the ODTRF’s Venture Grant program and was awarded $25,000 to investigate just that.
“We thought that by increasing the numbers of Tregs in transplanted patients, we could explore a new way to prevent organ rejection that wouldn’t come with the side effects of the immunosuppressive drugs that are currently used,” explains Megan.
Megan’s exploration proved very successful: she was the first in the world to show that these genetically engineered Tregs could be a powerful new therapy to stop harmful immune responses in transplantation.
“In 2016, I published a landmark paper on Tregs,” says Megan. “This publication on our new Treg-based therapy to improve the long-term success of organ transplantation resulted directly in a French company approaching me to take this idea to clinical testing. This collaboration allowed me to grow my lab and work much more intensely in this area, ultimately resulting in the first clinical trial of this concept. The seed funding from the ODTRF was the catalyst for this whole field of research.”
And what a field of research it is. With the use of engineered Tregs now in clinical testing, Megan’s current research is focused on creating the best-possible Tregs and finding ways to get them into the people who need them.
“The basic science of how these cells work excites me,” says Megan. “I am always working hard to learn more and better understand all that these cells are capable of.”
Alongside this work is Megan’s role in getting a flagship infrastructure project, the Advanced Therapeutics Manufacturing Facility, built on the UBC campus. This facility, spanning approximately 20,000 square feet, will support the production of advanced therapeutic products like vaccines, cell therapies and regenerative medicines.
“Ground broke on the facility at UBC in early November,” says Megan. “It excites me to think about what this building will bring to the university but also the far-wider ripple effect it will have that is way bigger than me.”
And what larger ripple effect than to have one’s work cited in the scientific background for the 2025 awarding of the Nobel Prize to “Immune tolerance: The identification of regulatory T cells and FOXP3”. (Megan’s lab’s work, which has its origins in the ODTRF grant, is the “Wardell et al” cited publication.)
“The $25k from ODTRF transformed my lab, and has grown into over $6 million in research support,” says Megan. “Indirectly everything connects back to that initial grant in 2011. I could have never imagined all that has come from it.”
Immunosuppression Reduction and the Risk of De Novo Donor-Specific Antibody Formation After Kidney Transplantation
From launching a precision medicine program, to a defining what makes a well-matched recipient and donor, to determining a pathway to drug minimization, to being one of the first labs in the world to embrace nanopore technology, Dr. James Lan’s pursuit of a new paradigm in transplant started with the ODTRF.
“What we found in our initial ODTRF funded project was that by six months after transplant, a great majority of patients had needed to reduce their anti-rejection medication as a result of toxicity,” explains James, a transplant nephrologist at Vancouver General Hospital and Medical Director of BC’s Immunology Laboratory. “The second thing we found was that when a patient’s dose was lowered, after a certain point, their chance of graft loss increased in the long term. This tells us that our medication, although effective, are not well tolerated.”
These were the catalyst for James and his team to launch a precision medicine program.
“We saw that when we cut down the dose to counter the medications’ negative impact, we start to expose patients to potential rejection and graft loss in long-term,” says James. “If we want to overcome this entire issue, we need to be more precise in understanding what’s the degree of mismatch between patient and donor.”
Next came a $10-million Genome Canada project grant, looking at the impact of mismatches between donor and patient as a re-stratification to guide immunosuppression. James’ mentor, Dr. Paul Keown, is the project’s Principal Investigator (PI), with James as lead investigator of this project pillar.
“We hypothesized that the patients who are the most vulnerable to develop these rejection issues are the ones who are not well-matched with their donor,” explains James. “We looked at the amino acid on the immune molecules that define patients and donors (called human leukocyte antigen (HLA)), and what we found is if the HLA molecules are very mismatched between patient and donor, the risk of rejection is higher.”
James notes that while this has been known for a long time, the advancement is the precision with which his lab is looking at very discrete amino acid residues on the molecules to determine a more exact measure of immune risk.
“The only way to try and counteract that risk is to give the patient more potent immunosuppressants,” says James. “But what we are now very aware of is the toxic nature of these meds. We are seeing more patients with not just infections, but also cancer related to chronic use of immunosuppressants. As people are living longer, their exposure to immunosuppression is also far longer than in early days of transplant.”
This awareness led to Dr. Keown’s (PI) and James’ (co-PI) next $3.6-million Genome Canada project: investigating kidney allocation.
“Right now, we allocate by waiting time; however, if we can also look at including matching, we can get more kidneys into better matched people,” says James. “We now know that recipients with well-matched organs won’t have the same issues with rejection, and this also offers a pathway for drug minimization so that we can avoid toxicities.”
Through his work, James and his team have now characterized, to a good understanding, what defines good matching and poor matching. “It is not straightforward but without that understanding, we cannot change how we allocate,” James notes.
In addition to this understanding, the second part to allocation is to be able to do it precisely, and quickly.
“If I want to be more precise in how I give drugs, and certainly if I want to allocate to someone well-matched on the waiting list, I need to be able to sequence the donor under very high resolution, and do compatibility assessments in real-time to precisely define the mismatches between the donor and patients, all within a few hours,” says James.
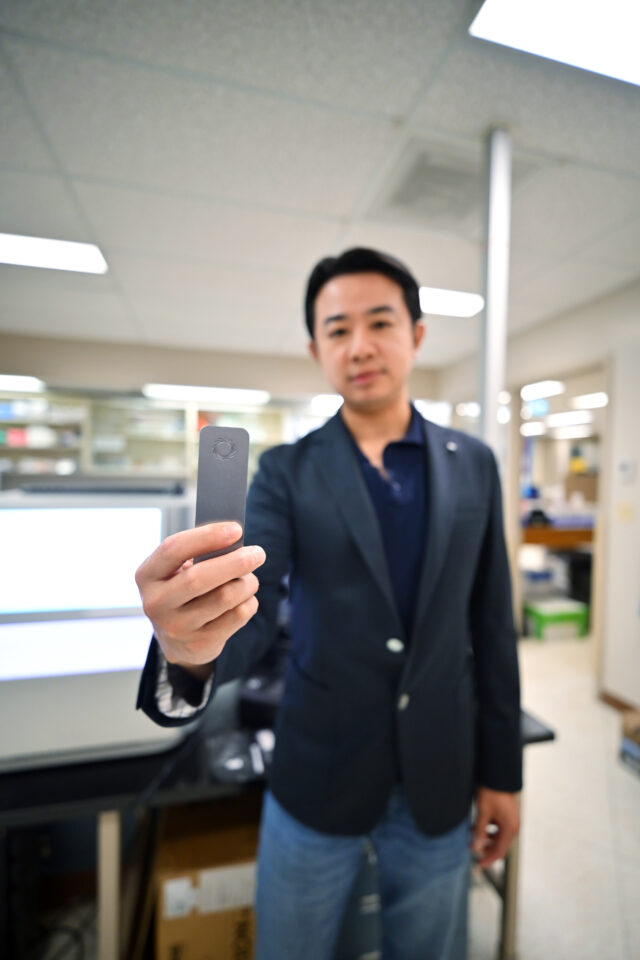
To aid in this precise rapid assessment, Dr. Lan’s lab has recently introduced what’s referred to as third generation sequencing. Using nanopore technology, you add donor DNA into a sequencer no larger than a cell phone, hook it up to laptop, and high-resolution sequencing is complete within a few hours.
“We are one of the first in the world to launch this new technology,” Dr. Lan says. “Technology advancement is what’s needed to drive the implementation of this strategy clinically.”
Ultimately, what drives this entire set of work – the potential for which was first realized through the research afforded via the ODTRF’s seed funding – is the belief that a new paradigm in transplant is needed.
“If we can improve the compatibility of these immune molecules between patients and donors, then that’s a pathway to minimize drugs and achieve the same good transplant outcomes – but hopefully without the same complications caused by chronic exposure to anti-rejection medication,” concludes James.
What Makes a Donation to the ODTRF Different?
“When you’re a scientist, chasing the next grant consumes you,” says Megan. “Simply having an idea that you want to explore makes it very hard to get funding. Typically, getting any sort of grant or funding is reliant on you having a body of work, proven results, to apply with. The ODTRF Venture Grant funding allowed me that; the seed funding was that start of everything for my lab.”
James notes the clear, critical role ODTRF plays, especially for early researchers, to aid in the development of proof-of-concept ideas that can be leveraged for larger funds.
“I am now mid-career, and without these early funding opportunities from the ODTRF and the ability to develop pilot data, we can’t land on these bigger ideas,” says James. “Many granting bodies look to fund established investigators, not explore new ideas. With seed funding, a lot of questions can be answered quickly. There are not many funding sources like the ODTRF that offer that preliminary support in transplantation research.”
Your donation to the ODTRF stays right here in BC, funding clinician researchers and investigators who are on the leading edge of donation and transplantation science. Your generosity could lead to the next huge breakthrough that helps us to support innovative organ donation and transplantation research to benefit the lives of organ recipients, living donors and caregivers, and improve the process for deceased donors and their families.
Donate Today!